Explore Any Narratives
Discover and contribute to detailed historical accounts and cultural stories. Share your knowledge and engage with enthusiasts worldwide.
The most brutal side effect of chemotherapy isn't nausea or hair loss. It's a silent, systemic theft. The very treatment designed to save a life can permanently rob the body of its ability to regenerate blood and immune cells, a condition known as stem cell exhaustion. For aging patients, a similar decline happens slowly, a creeping frailty rooted in faltering stem cells. The implications are vast: increased vulnerability to infection, anemia, and blood cancers. For decades, this decline was considered a one-way street, an immutable fact of biology and toxic treatment.
That street now has a U-turn.
In a cascade of discoveries through 2025 and 2026, scientists have not just slowed the aging of blood-forming stem cells—they have reversed it. They are hitting rewind on cellular time. The work is happening not with speculative gene editing, but with precise molecular tools targeting the fundamental machinery that goes awry as cells age. This isn't about extending lifespan on a calendar; it's about forcibly restoring healthspan at the cellular level, with profound implications for millions undergoing chemotherapy and grappling with the diseases of old age.
Deep within our bone marrow, hematopoietic stem cells serve as the mother lode for our blood and immune systems. They are prolific, but not immortal. With age and stress, their performance plummets. The search for the master switch behind this decline led a team at the Icahn School of Medicine at Mount Sinai to a surprising culprit: the lysosome.
Think of a lysosome not as a simple wastebasket, but as a high-tech cellular recycling center. It breaks down worn-out components, extracting raw materials for reuse. In aged blood stem cells, this center goes haywire. It becomes hyperactive and overly acidic, like a recycling plant burning through material too fast and spewing toxic fumes. The Mount Sinai team, in work published in early 2025, made a radical decision. Instead of boosting this degraded system, they slowed it down.
They treated aged stem cells from mice with a lysosomal inhibitor, a compound that temporarily puts the brakes on this frenetic recycling. The result was not further decay, but rebirth. The treated stem cells, when transplanted, demonstrated an over eightfold increase in their blood-forming capacity compared to their untreated aged counterparts. They began functioning like young cells again. The mechanism was elegant: by calming the lysosome, the team reduced the leakage of mitochondrial DNA fragments, which are mistaken by the cell as signs of viral invasion. This dampened the hyperactive cGAS-STING immune alarm pathway—a key driver of the chronic inflammation that characterizes aged stem cells.
We effectively reset the aged stem cells to a younger functional state by correcting a fundamental defect in their waste processing. This isn't a cosmetic fix. We observed a true restoration of regenerative potential, achieved by targeting the root cause of the inflammatory signaling that cripples these cells with age.
The lead investigator on the Mount Sinai study, whose team's findings were released in March 2025, frames it as a fundamental correction. The quote, translated from the original research announcement, captures the paradigm shift: this is root-cause medicine for cellular aging.
While one team focused on cellular recycling, another pinpointed a specific protein acting as a throttle on aging. RhoA, a signaling protein, exists in every cell. In a study detailed in Nature Ageing in late 2025, researchers found RhoA in a state of constant, hyperactivity in aged blood stem cells. It was as if the protein was stuck in the "on" position, sending relentless signals that disrupted normal function and division.
The team had a weapon: a small, drug-like molecule named Rhosin, designed specifically to inhibit RhoA. They took aged blood stem cells, treated them with Rhosin ex vivo—outside the body in a lab dish—and then transplanted them. The treated cells displayed improved molecular markers of youth and, critically, a significantly enhanced ability to repopulate the bone marrow and produce healthy blood lineages. The approach was different from the lysosomal strategy, but the goal was identical: identify a specific, dysregulated component of aged cells and forcibly reset it.
What does this look like in practical terms? Imagine a future where, before a patient undergoes harsh chemotherapy, a sample of their healthy blood stem cells is harvested and banked. After treatment, those cells aren't just reinfused as-is. They are first treated in a lab with a rejuvenating cocktail—perhaps a lysosomal inhibitor, a dose of Rhosin, or something else entirely—to repair the accumulated damage of age and preempt the toxic assault of the drugs. They are then returned to the patient, not as depleted survivors, but as fortified reinforcements.
Our work with RhoA inhibition shows that cellular aging is not a mysterious fog. It is a series of discrete, targetable pathways. Turning down RhoA activity is like releasing a brake on the stem cell's regenerative potential. The fact that we can do this with a small molecule opens very clear doors for therapeutic development.
A principal author of the RhoA study, commenting on the findings in September 2025, emphasized the druggable nature of the target. The translation from the original scientific commentary highlights the clinical practicality researchers are now chasing.
The race is no longer just to understand aging. It is to interrupt it. And as these first two approaches demonstrate, the interrupt signals are being found in the most mundane of cellular places: a waste processor, a common signaling protein. The third major player, however, comes from outside the stem cell entirely. It arrives in the mail.
Researchers at the University of Illinois Chicago took a different tack. They looked for a factor in young blood that could instruct old stem cells. In 2026, they identified platelet factor 4 (PF4), a protein released by platelets, as a powerful instructor. When they gave aged mice daily infusions of PF4, the effects cascaded through their systems. Their blood stem cells, and the immune cells they produced, began to look and behave like those from much younger animals. The inflammation characteristic of old age receded. The effect was so potent that simply adding PF4 to aged human stem cells in a dish triggered a similar rejuvenation.
One therapy targets internal waste management. Another silences a noisy protein. The third delivers a youthful memo via the bloodstream. The convergence is the story: aging is reversible from multiple angles. The scientific consensus, hardened in the last two years, has pivoted from "if" to "how soon." The remaining question is whether these laboratory triumphs can survive the brutal journey to the clinic, and for whom they will work first.
The proof of concept is undeniable. Aged and exhausted blood stem cells can be made young again in a dish. The scientific triumph, however, is the easy part. The real story now is the chaotic, competitive, and wildly ambitious scramble to translate these lab reversals into clinical treatments. This phase is less about elegant biology and more about manufacturing, delivery, and a fundamental debate over strategy. Should we tweak cells inside the body or rebuild them outside? Is the goal a gentle nudge or a hard reset?
The landscape has fractured into distinct camps, each armed with different tools and philosophical approaches to cellular rejuvenation.
One faction, exemplified by work emerging from Tel Aviv University, is betting on precision messaging. Their tool is mRNA technology, familiar from COVID-19 vaccines, but aimed at a far more complex target. Instead of instructing muscle cells to make a viral spike protein, their approach designs mRNA to precisely reactivate dormant genetic programs within hematopoietic stem cells (HSCs). The goal is to "wake up" the stem cells' intrinsic ability to proliferate and differentiate, effectively regrowing a blood and immune system from the inside out. This is an in vivo strategy—treating the patient, not just their extracted cells.
"This approach opens up new avenues for therapeutic interventions for patients who have lost bone marrow due to chemotherapy or disease. We are not just supporting cells; we are sending them a direct command to rebuild." — Researchers at Weill Cornell Medicine, commenting on the mRNA-based regeneration approach.
The appeal is surgical specificity and the avoidance of viral vectors, which have long carried a latent risk of triggering cancer. But delivering mRNA to the exact right stem cells, nestled deep in the bone marrow niche, presents a delivery challenge of monumental scale. Is a lipid nanoparticle smart enough to find its target? The optimism is palpable, but the technical hurdles are vertical.
Contrast this with the ex vivo, or "outside-the-body," faction. Here, the process is more industrial. Stem cells are harvested, processed in a controlled laboratory environment—often using 3D culturing systems or precise chemical baths—and then reinfused. This is where the lysosomal inhibitors and Rhosin molecules from earlier studies shine. It's also where a quieter revolution is happening with extracellular vesicles (EVs).
Think of EVs as tiny biological packages mailed from one cell to another. A 2025 study in Stem Cell Research & Therapy demonstrated that EVs derived from mesenchymal stem cells could dramatically boost tissue repair. The numbers are stark: treatment resulted in a 44% increase in collagen, a 68% jump in elastin, and a staggering 113% rise in hyaluronic acid production. For blood stem cell support, the principle is similar. These nanoscale parcels can deliver rejuvenating signals—proteins, RNA, enzymes—directly to aged HSCs, potentially resetting them without ever removing them from the body. Companies are already commercializing this, with protocols like "Cell Factor" using DNA-free EVs designed to cross the blood-brain barrier and enact systemic effects.
"The main limitation of autologous therapy has always been the reduced potency of the patient's own aged cells. Rejuvenation via exosomes or 3D culture offers immense potential for degenerative diseases, but it absolutely requires us to optimize the niche factors and account for donor health." — Analysis from a 2025 PMC review on autologous stem cell therapy.
This quote cuts to the core logistical nightmare. Autologous therapy—using a patient's own cells—is safer from an immune rejection standpoint. But what if the patient is 75 years old and ravaged by chemotherapy? Their cells are the problem. The entire ex vivo rejuvenation industry hinges on making a silk purse from a sow's ear, and the success rate is not yet guaranteed.
While academics debate mechanisms, the clinic moves forward on parallel tracks. On a concrete date—November 2024—a clinical program at Keio University in Japan, using products manufactured by ReproCELL, began patient dosing of tumor-infiltrating lymphocyte (TIL) therapy for cervical cancer. This isn't straight HSC rejuvenation, but it's a close cousin in the regenerative immunotherapy family. The therapy involves expanding a patient's own immune cells, a process that relies on healthy hematopoietic support. It's a stepping stone, proving the large-scale manufacturing and reinfusion protocols that any ex vivo blood stem cell therapy will need.
More audacious are the plays for off-the-shelf, universal therapies. ReproCELL and others are racing to develop HLA-knockout induced pluripotent stem cells (iPSCs). The vision is a bank of "universal donor" stem cells that could be differentiated into blood stem cells for any patient, eliminating the harvest-and-repair bottleneck entirely. The Lund Stem Cell Center champions the superiority of iPSC-derived mesenchymal stem cells, noting their "superior homogeneity and reproducibility" compared to traditionally sourced MSCs. It's a factory model versus an artisanal one.
But does pushing cells back to a pluripotent state, only to redirect them, introduce its own dangers? The epigenetic landscape of an iPSC is a blank slate, and ensuring it fills in correctly every single time is a monumental quality control challenge. The field is littered with the ghosts of therapies that worked beautifully in clonal populations but failed in the messy heterogeneity of human trials.
"mRNA technology allows us to precisely 'wake up' hematopoietic stem cells. This could revolutionize treatment for blood cancers and bone marrow failure." — Tel Aviv University research team on their breakthrough approach.
The revolution is always imminent. Yet, for every vocal optimist, there is a cautious pragmatist working in the background. Researchers publishing in BMB Reports warn that epigenetic interventions—using drugs to alter DNA methylation or histone acetylation patterns—must be "transient and pulsed" to avoid overwhelming cellular machinery and triggering a stress response that could be worse than the original aging. You can't just blast an old cell with youthful signals and expect it to cope. It's a dialogue, not a shout.
This is the central, often unspoken, tension in the field: the battle between aggressive reprogramming and gentle modulation. The mRNA and iPSC camps lean toward the former; the EV and lysosomal inhibitor camps toward the latter. My money, for what it's worth, is on the gentle modulators for first-generation success. The body rejects brute force. The history of medicine is a history of therapies that mimicked natural processes, not overwrote them.
Let's be brutally practical. A therapy can make a stem cell 50% more effective, but if you start with ten nearly-dead cells, you end up with fifteen mediocre ones. This is the numbers game. Some clinics, like Liv Hospital, highlight the use of "afterbirth marrow"—stem cells from umbilical cord blood and tissue—as a potent, young source to complement these rejuvenation strategies. It's a hybrid model: boost the old system with a fresh, young graft. It's not as scientifically sexy as reversing aging in situ, but it might get a patient out of the hospital faster.
Other strategies focus on expansion. FLI-1 protein research aims to multiply HSCs in culture, making bone marrow transplants more efficient. But expansion risks exhaustion. You can only force a cell to divide so many times before it hits its Hayflick limit and gives up. The true solution likely lies in the niche—the microenvironment of the bone marrow that cradles and instructs stem cells. A rejuvenated cell placed back into a decayed, inflammatory niche is like planting a healthy seedling in poisoned soil. The niche is the next frontier, and it's fiendishly complex to engineer.
"Epigenetic modulators can restore a more youthful landscape in HSCs, but the interventions must be carefully timed. It's not an on/off switch you can leave flipped." — Cautionary perspective from BMB Reports on epigenetic rejuvenation.
So where does this leave the patient today? In a frustrating limbo. The cascade of discoveries in 2025 and 2026 is real, but the "cascade" of available treatments is not. The most advanced applications are still in adjacent fields: TIL therapy for cancer, EV treatments for cosmetic and orthopedic repair. The direct, approved "stem cell rejuvenation injection" for chemo patients or the elderly does not exist. The gap between a stunning Nature Aging paper and a vial in a pharmacy is a chasm measured in years, billions of dollars, and regulatory agony.
The critical analysis here is unavoidable. The field is overheating with hype, fueled by venture capital and the powerful, human desire to conquer aging. The preprint servers are flooded with miraculous mouse studies. The press releases promise revolutions. Yet, the clinical trial registries tell a slower, more grinding story. The translation from mouse to human is historically brutal, especially in immunology and stem cell biology. A mouse is not a man. Its lifespan is compressed, its immune system simpler, its biology a useful but flawed model.
What works? Targeted, ex vivo approaches for specific conditions—like repairing a cancer patient's own cells before a transplant—have the clearest path. They are controllable. What doesn't? The notion of a single, systemic "youth shot" that comprehensively reverses blood stem cell aging in a 70-year-old. Biology is too interconnected, too redundant, and too stubborn for that. The future is combinatorial: a shot of PF4 to calm inflammation, an infusion of engineered EVs to deliver repair instructions, maybe a temporary epigenetic drug to clear molecular clutter. It will be a regimen, not a miracle.
The skeptics are right to demand more human data. The optimists are right to champion the staggering pace of discovery. The patients, caught in between, have every right to demand that the field channel its chaotic energy into rigorous, transparent, and patient-centered clinical progress. The science has delivered hope. Now the hard work of delivering medicine begins.
The true weight of blood stem cell rejuvenation isn't measured in lab assays or mouse survival rates. It’s measured in the dismantling of a core dogma of medicine: that aging and cumulative damage are linear, irreversible processes. For a century, gerontology and oncology operated on a principle of managed decline. We could cut out a tumor, we could support a failing system, but we could not roll back the cellular clock that made tissues vulnerable in the first place. This research declares that principle obsolete. The impact is not merely therapeutic; it is philosophical, forcing a rewrite of medical textbooks and, more profoundly, our narrative of human longevity.
It shifts the goal from lifespan—adding years to life—to healthspan, adding life to years. The economic and social implications are staggering. A 2025 review in a prominent clinical medicine journal framed it not as a niche hematology story, but as a systems-level intervention. If you rejuvenate the blood and immune system, you don't just prevent anemia or blood cancers. You potentially alter the course of Alzheimer's disease, where neuroinflammation is fueled by aged immune cells. You change the prognosis for cardiovascular disease, where inflammatory monocytes damage arterial walls. You rebuild resilience against infections that kill the elderly. The hematopoietic stem cell is a master regulator, and resetting it sends corrective signals throughout the entire biological network.
"We are moving from a paradigm of replacement—transplanting new stem cells—to one of restoration. This is a fundamental shift. It acknowledges that the patient's own biology, given the right instructions, retains the capacity for profound self-repair, even after profound insult." — Director of Regenerative Medicine at a leading European stem cell center.
This quote, translated from a recent symposium on clinical translation, captures the cultural shift within medicine itself. The patient is no longer a passive recipient of foreign cells or toxic drugs, but an active site of renewable potential. It’s a more empowering, if more technically demanding, model of care. The legacy of this work will be judged not by the first rejuvenated mouse, but by the first generation of chemotherapy patients who receive their own fortified stem cells back, sidestepping the devastating exhaustion that currently defines cancer survivorship.
For all the promise, the field is not a parade of triumphs. It is a minefield of valid, serious criticisms that its champions cannot ignore. The first is the hype cycle. The term "rejuvenation" itself is a double-edged sword, dripping with the promise of eternal youth and exploited by unscrupulous clinics offering unproven "stem cell facelifts." This legitimate science risks being drowned in a sea of pseudoscience and patient exploitation. Every overstated press release from a university tech transfer office fuels a predatory industry waiting to mislead the desperate.
The second criticism is one of staggering inequality. These therapies, if and when they arrive, will be astronomically expensive. The ex vivo processing, the GMP manufacturing, the personalized molecular cocktails—this is not a cheap pill. We are sketching a future where the wealthy can purchase decades of renewed immune function, while the public health systems buckle under the cost. The technology could become the ultimate biomarker of socioeconomic divide, not just in lifespan, but in the quality of healthspan.
The most damning scientific criticism, however, targets biological naivete. The focus on the hematopoietic stem cell, while logical, may be myopic. Aging is a systemic phenomenon. Rejuvenating blood stem cells and placing them back into an aged body with stiffened arteries, a leaky gut, and a senescent tissue microenvironment is like putting a new engine into a rusted-out chassis. The inflammatory signals from the rest of the aged body will quickly stress the renewed cells. The niche matters. The 2025 PMC review explicitly noted that donor health and "niche factors" are critical, yet largely unaddressed, limitations. Without concurrent strategies to rejuvenate the bone marrow microenvironment and systemically reduce inflammation, the effects of HSC rejuvenation alone may be transient, a beautiful but fleeting correction.
Finally, there is the specter of unintended consequences. Epigenetic reprogramming, while reversible in theory, could open chromatin in dangerous places, accidentally activating oncogenes. Forcing aged cells to proliferate vigorously could simply accelerate their journey toward malignancy. The field remembers the lessons of gene therapy's early days, when curing one disease inadvertently caused another. The caution from BMB Reports about transient, pulsed interventions is a warning born of that history. The race to rewind time must not become a race to trigger cancer.
The path forward is not a straight line to a miracle cure. It is a series of concrete, cautious steps. Look for the next milestones not in flashy headlines, but in clinical trial registries. The first Phase I trials specifically testing lysosomal inhibitors or RhoA antagonists on human hematopoietic stem cells are likely to be announced before the end of 2026. The ReproCELL and Keio University TIL therapy program will publish its first efficacy data for cervical cancer patients in late 2026 or early 2027, providing a crucial proof-of-concept for the large-scale cell manufacturing and reinfusion logistics that blood stem cell therapies require.
The most immediate application will be in the bridge-to-transplant setting. By 2028, expect the first published studies where chemotherapy patients' own harvested stem cells are treated ex vivo with a rejuvenating agent before autologous transplant, with the primary endpoint being the speed of neutrophil and platelet recovery. Success here will pave the way for broader indications. The prediction, based on the current pipeline, is that regulatory approval for a specific, narrowly defined use—like preventing stem cell exhaustion in high-dose chemotherapy for lymphoma—will arrive around 2030. The universal, off-the-shelf iPSC-derived blood stem cell is a 2035 prospect, at the earliest.
These dates are not guesses; they are extrapolations from the current glacial pace of cell therapy trials. They are a reminder that biology’s complexity imposes its own timeline. The silent theft that begins with a chemo infusion or the slow creep of years may finally meet its match. Not with a shout, but with a series of precise, molecular whispers, telling old cells to remember what it was like to be young.
In conclusion, the emerging science of rejuvenating blood stem cells offers a beacon of hope for countering the devastating effects of chemotherapy and aging. This pivotal research compels us to support and accelerate its translation into clinical therapies that could redefine recovery and longevity.







Your personal space to curate, organize, and share knowledge with the world.
Discover and contribute to detailed historical accounts and cultural stories. Share your knowledge and engage with enthusiasts worldwide.
Connect with others who share your interests. Create and participate in themed boards about any topic you have in mind.
Contribute your knowledge and insights. Create engaging content and participate in meaningful discussions across multiple languages.
Already have an account? Sign in here

На МКС успешно напечатали 8 нервных имплантов в микрогравитации — прорыв, который может изменить лечение травм спинного ...
View Board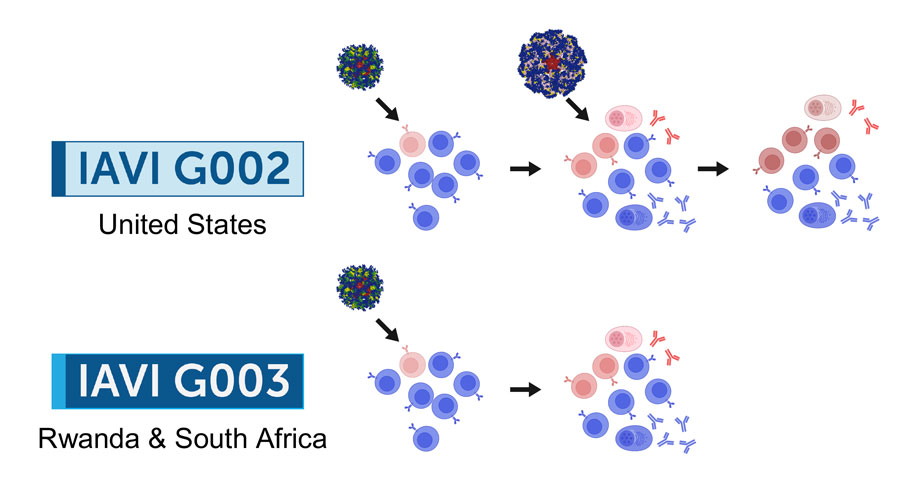
2026 marks a pivotal year for mRNA tech, with breakthroughs in cancer, HIV, microneedles, and AI-driven trials set to re...
View Board
After a stroke, 58‑year‑old Altia Bryden woke speaking fluent Italian, revealing rare Foreign Accent Syndrome and its pr...
View Board
Major 2025 trials reveal no effective treatments for long COVID brain fog, forcing a shift from cognitive training to im...
View Board
MIT chemists synthesize verticillin A after 55 years, unlocking a potential weapon against fatal pediatric brain tumors ...
View Board
Cancer research reaches new heights as ISS microgravity enables breakthroughs like FDA-approved pembrolizumab injections...
View Board
Scientists capture influenza virus invading a human cell in real-time using groundbreaking ViViD-AFM microscopy, reveali...
View Board
AI revolutionizes medical physics, crafting precise radiation plans in minutes, transforming diagnostics, and reshaping ...
View Board
Pancreatic cancer's sugar-coated shield uncovered: Researchers reveal how tumors exploit sialic acid to deceive immune c...
View Board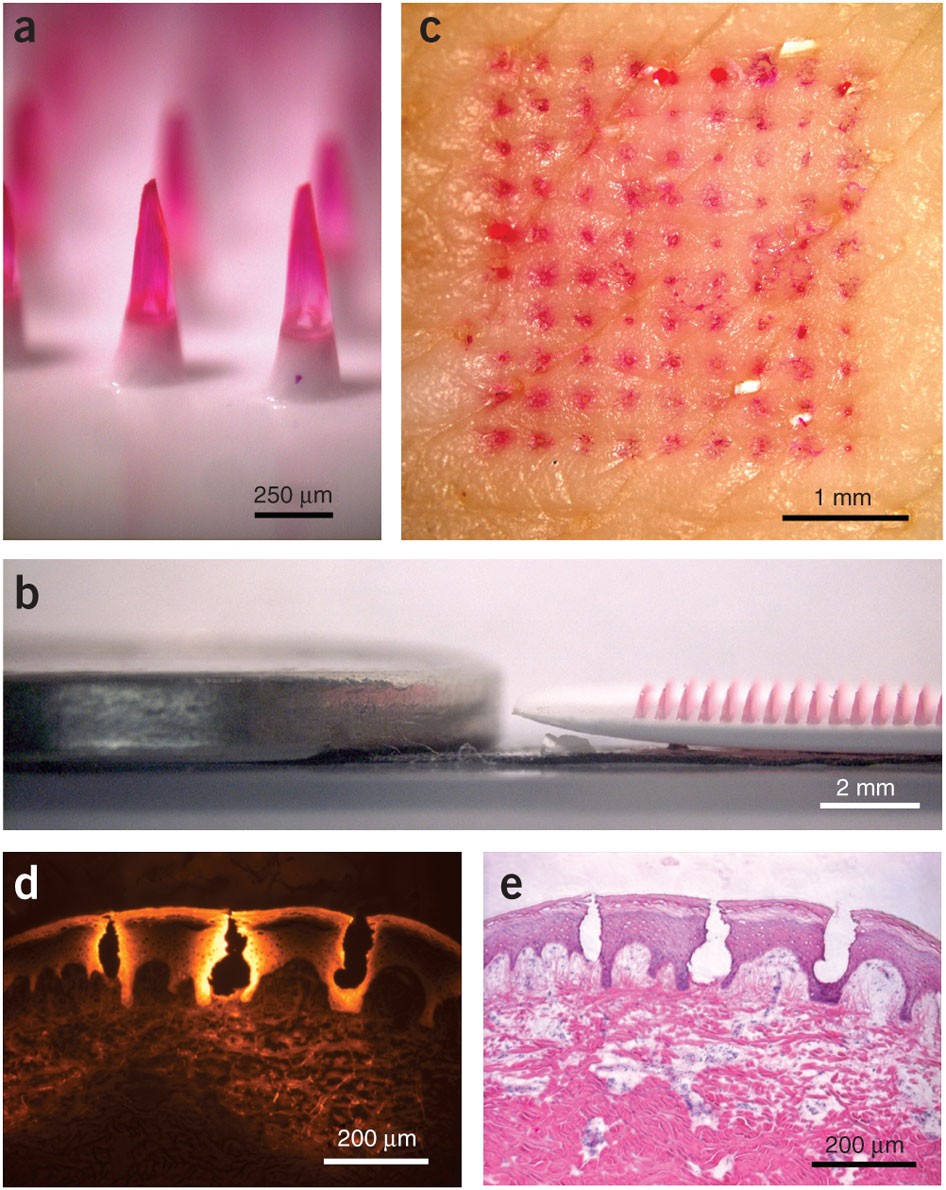
Microneedle patches deliver painless, effective vaccines via skin, revolutionizing global healthcare with self-administr...
View Board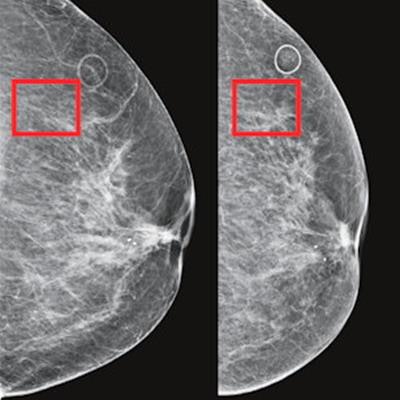
AI-powered cancer screening transforms early detection, with clinical trials showing a 28% increase in cancer detection ...
View Board
Michelle Phan and the Algorithm of Authenticity The year is 2007. YouTube is two years old, a platform dominated by sha...
View Board
Resucitan genes de mamut en laboratorio: científicos en Texas logran crear ratones con pelaje lanudo, un paso crucial pa...
View Board
Radiation-driven wolves in Chernobyl display rapid cancer-resistant evolution, a 30-year natural experiment revealing ge...
View Board
AI transforms healthcare in 2026, detecting hidden tumors, predicting diseases before symptoms, and personalizing treatm...
View Board
Sea of Thieves: An Epic Adventure on the High Seas Picture this: the horizon is a molten orange line against a deepenin...
View Board
Archaeologists uncover Belize's first Maya king, Te K’ab Chaak, in a 1,700-year-old tomb, rewriting Caracol’s origins wi...
View Board
Nel 2026, l'Intelligenza Artificiale Agente rivoluzionerà il lavoro: da semplice esecutore a pianificatore autonomo, con...
View Board
The open AI accelerator exchange in 2025 breaks NVIDIA's CUDA dominance, enabling seamless model deployment across diver...
View Board
Alan Melikdjanian: The Skeptic's Visual Effects Architect The internet is a carnival of the bizarre and unbelievable. A ...
View Board
Comments